Experiencing Rural Morocco Through Healthcare
Lydia George
Dr. Amy Way*
Lock Haven University
Abstract
An international service-learning program to Morocco consisted of students and faculty from Lock Haven University and was conducted in 2009, 2010, 2012, and 2014 for a week at a time. Data was collected from different populations in Morocco and was analyzed based on the populations’ height, weight, BMI, blood pressure, and chief complaints. The populations were then compared to each other, to the national health of Morocco, and to the United States.
Introduction
For many years, Lock Haven University has provided learning opportunities for students to travel to and serve international communities. Service opportunities have included building houses, creating maps of the area, and providing basic health care. Over the last few years, interest in offering health science service-learning programs has grown. In 2009, a group of undergraduate students along with physician assistant graduate students traveled to Tighfist, Morocco, a remote location in the High Atlas Mountains. As part of their service to the Moroccans, these students collected weight, height, gender, and age data to assess the Tighfist population. Returning again in 2010, the service team from Lock Haven expanded their data collection by including blood pressure, pulse, and hemoglobin recordings.
Subsequent service-learning programs took groups to a different area in Morocco called the Skoura Oasis, located in a remote area of the Northern Sahara Desert. In 2012 and 2014, groups included in their data collection pulse, respirations, and blood pressure in addition to height, weight, age, and gender.
The collected data from these two areas is important to the growth and development of healthcare programs and education in remote populations of Morocco by creating a profile of the health status of rural areas. Currently in Morocco, most health providers and health care centers are located in urban areas (World Health Organization, 2006). Outpatient care is provided to rural areas through traveling medical teams and pharmacies. Different organizations such as the World Health Organization, the Ministry of Public Health, and UNICEF support the Moroccan government in reducing widespread diseases and these organizations have made great strides in reducing diseases such as tuberculosis and malaria (World Health Organization, 2006). However, there is still a need for education in prevention of diseases such as high blood pressure, diabetes, and obesity in adults and malnutrition in children.
This study included two populations: Tighfist in the High Atlas Mountains and Skoura in the Northern Sahara Desert. The first aim for this study was to compare the Skoura Oasis population located in the desert of Morocco to the population in Tighfist of the High Atlas Mountains. Next, this study sought to compare Tighfist and Skoura based on health averages. Blood pressure, BMI, height, weight, and physicians notes were compared between the two remote populations of Morocco. The next objective was to compare these two villages of Morocco to national averages. The last goal of this study was to evaluate health differences between the people of Tighfist and Skoura in Morocco to the health of Americans in the United States. We were able to compare BMI, blood pressure, height, and weight between the two populations.
This study on Tighfist and Skoura was important to assess the major health issues in rural areas of Morocco and determine what we can do to serve the populations in rural Morocco in future programs.
Methods
Over the course of the Fall 2014 semester, after the study was approved by the Institutional Review Board to protect the rights of human subjects, data from four years of service learning programs to Tighfist and the Skoura Oasis were compiled and sorted. Data slips ranging from pieces of notebook paper to full physical assessment sheets have been taken into account for this study. The compiled data slips are from 2009 in Tighfist, 2010 in Tighfist, 2012 in the Skoura Oasis and 2014 in Skoura Oasis. The first service-learning program to Tighfist in 2009 collected data on pieces of notebook paper. These collections included height, weight, gender, age, and sometimes physician’s notes. In 2010, the trip to Tighfist also collected data on pieces of notebook paper which included gender, height, blood pressure, and weight for most individuals but did not include age. Based on the average of ages of individuals from the Skoura Oasis, we have estimated individuals from Tighfist as being a child or an adult to allow for inclusion of this data, despite the lack of information on the Tighfist individuals’ ages.
The first trip to the Skoura Oasis in 2012 used assessment sheets that included gender, age, height, weight, pulse, blood pressure, respirations, and doctors’ notes for most individuals. Finally, the second trip to the Skoura Oasis in 2014 used physical assessment sheets that included age, gender, height, weight, pulse, pulse ox, blood pressure, and doctors’ notes for most individuals.
We were able to calculate averages for the following data: BMI, blood pressure, height, weight, and pulse for most individuals. Additionally, we were able to document common health issues in Morocco because of physicians’ notes on the data slips.
An organization called Knoema compiles data sets from other organizations into databases to make research easier for individuals to find and reference. This database includes data sets from the World Health Organization (WHO) for global BMI classifications. The WHO classifies adults with a BMI less than 18.5 to be underweight, individuals with a BMI between 18.5-24.99 normal, adults with a BMI greater than 25.00 to be overweight, and BMI greater than 30 to be obese (Knoema, 2014). These values were used to determine the classifications of BMI of the populations that were studied.
We used percentiles from the Centers for Disease Control and Prevention (CDC) to classify BMI of the children in Tighfist and Skoura (Centers for Disease, 2014). Since age was not included for any of the children in Tighfist or Morocco, we used averages based on the age of 10 for males and females from our other data collections. BMI was calculated and the children of these areas were placed into a category (Table 1).
| BMI Percentile | Range | Classification |
| 3rd | <14.1- 14.36 | Underweight |
| 5th | 14.37-14.7 | Underweight |
| 25th | 15.6-16.8 | Healthy |
| 50th | 16.9-18.4 | Healthy |
| 75th | 18.6-19.6 | Healthy |
| 85th | 19.7-20.6 | Healthy |
| 90th | 20.7-22.5 | Overweight |
| 95th | 22.6-24.2 | Overweight |
| 97th | 22.7- ≤24.3 | Obese |
Table 1. Weight classification of children based on BMI percentile.
To determine hypertension in our populations, we based our standards on a previous study done in Morocco. The Pan African Medical Journal in 2012 evaluated the prevalence of hypertension in diabetic Moroccans. During this study, they classified an individual as hypertensive if their systolic blood pressure was ≥ 140 mmHg and diastolic blood pressure was ≥ 90 mmHg (Berraho, et al., 2013). These values were used as a basis for comparison in the two populations to determine whether or not the individuals in Skoura and Tighfist are hypertensive.
Results
Currently, we have enough data to calculate Body Mass Index (BMI), a simple calculation that relates height and weight to assess underweight, overweight, and obesity. BMI is used to assess population-level body weight and is defined as an individuals weight in kilograms divided by their height in meters squared. Although this is not the most efficient way to assess an individual’s amount of fat, BMI will be used because that is the data available from the service-learning programs (Centers for Disease, 2014). As can be seen in figure 1a, 68 adults had a recorded height, weight, and gender in Tighfist in 2009. 75% of males and 93.3% of females fit into the internationally ranked underweight category. This demonstrates that the majority of males and females were considered to be underweight in this data collection from 2009. Figure 1b shows the data collection from Tighfist in 2010. This collection includes 84 adults: 66.7% of males and 57.1% of females. The greatest majority for both genders ranked in the underweight BMI category. In the data collection from 2012 in Skoura, the largest percentage of individuals, 70.8% of males and 54.3% of females, are of normal Body Mass Index classification. There were 332 individuals included in this collection: 65 males and 267 females (Figure 2a). There were 56 total (22 male, 34 female) adults from the 2014 Skoura Oasis service-learning program with a recorded height, weight, and age. Again, the largest percentage out of all of the males was 72.7%, this group was considered to have a normal BMI. The females were 35.3% normal and 38.2% overweight in Skoura in 2014 (Figure 2b).
Figure 1: BMI classifications from the first data collection in Tighfist in 2009 (1a) and from individuals in Tighfist in 2010 (1b).
1a.
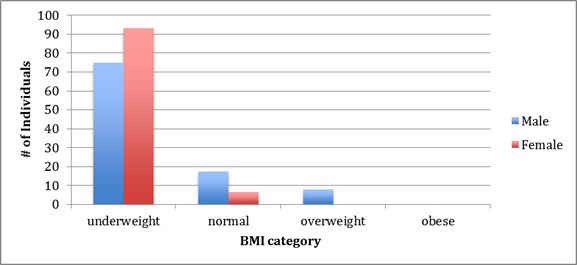
1b.
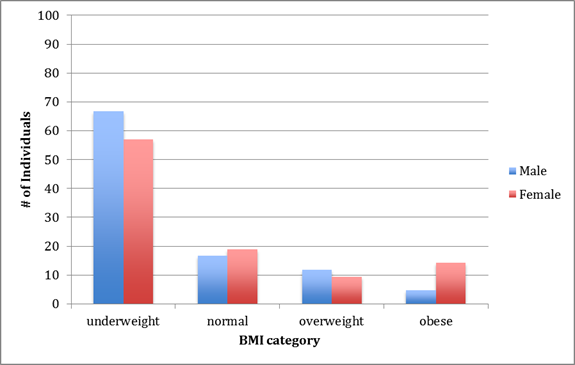
Figure 2: BMI categories for adults in the 2012 Skoura collection (2a) and adults from the 2014 Skoura Oasis service-learning program with a recorded height, weight, and age. (2b).
2a.

2b.
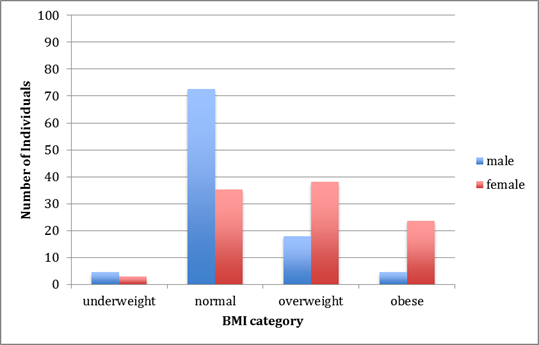
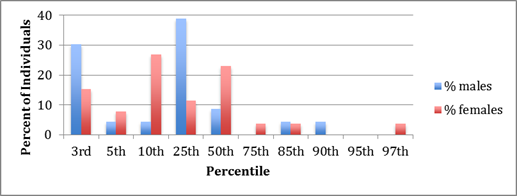
Each child in the data collections that had a recorded height and weight received a classification of being in either the 3rd, 5th, 10th, 25th, 50th, 75th, or 90th percentile based on the Center for Disease Control’s Body Mass Index values. In the data collection from 2009 in Tighfist, there were 54 total children: 23 males and 31 females. The largest majority of the female children ranked in the 10th percentile while the largest majority of male children ranked in the 25th percentile (Figure 3a). We did not have any individuals that fit into the 95th and 97th percentile. Unfortunately we did not have enough data on children from the 2010 Tighfist trip so a graph is not included on these individuals. In the data collection from the service-learning program to the Skoura Oasis in 2012, there were 169 total children, 88 males and 81 females. For both genders, the greatest percentage of children is in the 25th percentile (Figure 3b). The 25th percentile is considered to be healthy based on international Body Mass Index classifications. Next, children in the 2014 Skoura data collection were also classified based on Body Mass Index. The greatest number of individuals for females and males fall into the 10th and 25th percentiles, respectively (Figure 3c). These percentiles are considered healthy, but are closer to being underweight as opposed to overweight.
Figure 3: BMI percentile categories for children in the 2009 Tighfist collection (3a), children in the Skoura 2012 data collection (3b) and BMI percentile classifications for children in the 2014 Skoura data collection. (3c).
3a.

3b.
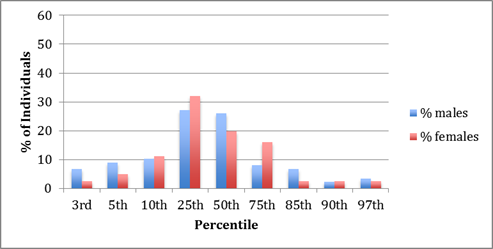
3c.
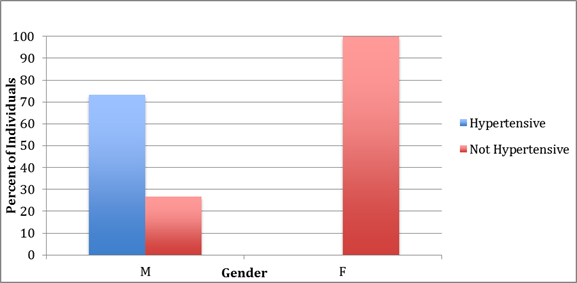
Finally, hypertension was analyzed based on prevalence in each of the rural populations. In the Tighfist population, all of the females that had blood pressure data on their data sheet did not have hypertension while 73.3% of males in these populations were hypertensive (Figure 4a). This collection is based on 25 individuals: 10 females and 15 males. Average systolic blood pressure in this population was 126.48 and the average diastolic blood pressure was 72.64. Hypertension in adults in the 2012 and 2014 Skoura Oasis data collection was also analyzed. There were 385 adults: 86 males and 299 females. As you can see from the graph, 52.3% of males and 28.5% of females were hypertensive (Figure 4b). This shows that almost half of all males in Skoura Oasis that were seen in the clinic were hypertensive and about a quarter of the women were hypertensive as well. Average systolic and diastolic blood pressure values were calculated for both populations (Table 2).
Figure 4: The prevalence of Hypertension in Tighfist adults from the 2009 and 2010 data collections (4a) and hypertension in adults in the 2012 and 2014 Skoura Oasis data collection (4b).
4a.
4b.
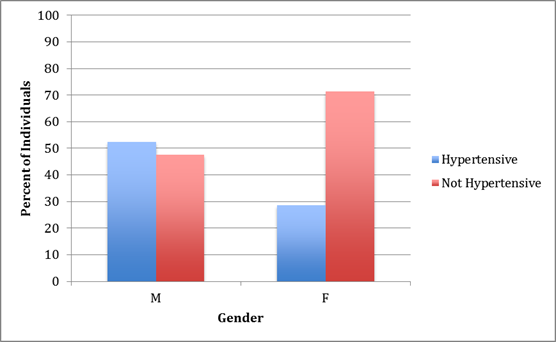
Table 2. Average for diastolic and systolic blood pressure collections in Tighfist and Skoura.
| Location | Type | Average |
| Skoura | Systolic | 136.3 |
| Skoura | Diastolic | 77.3 |
| Tighfist | Systolic | 126.5 |
| Tighfist | Diastolic | 72.6 |
The final average calculated was the average heights and weights of individuals in the Skoura and Tightfist populations (Table 3). Throughout the data collection, physician/physician assistant notes on the data slips were recorded along with the numerical data in an Excel spreadsheet. The most prevalent issues recorded on the data slips were goiters, eye abnormalities, and tonsil abnormalities (Table 4). Based on this data, the next program that travels to Morocco could focus on factors that affect eye health such as dust, debris, or work sites. The next service-learning program could also focus on ways for individuals with goiters to increase their iodine intake and to educate the people on the condition. Finally, the group could focus on the close proximity of the tonsils of the people from Tighfist and see if this is a biological abnormality or a precursor to sickness.
Table 3. Average female and male heights and weights in Tighfist and Skoura.| Place and Year | Goiter | Tonsils | Eye |
| Tighfist 2009 | 10 | 14 | 0 |
| Tighfist 2010 | 24 | 21 | 15 |
| Skoura 2012 | 1 | 2 | 8 |
| Skoura 2014 | 5 | 9 | 6 |
Table 4. Incidence of goiter, tonsils, and eye abnormalities in each year of the study.
| Age | Gender | Location | Average Height | Average Weight |
| Adult | Male | Skoura | 166.5 | 64.1 |
| Adult | Female | Skoura | 155.6 | 60.3 |
| Adult | Male | Tighfist | 141.2 | 39.8 |
| Adult | Female | Tighfist | 139.7 | 39.7 |
| Child | Male | Skoura | 109.6 | 20.6 |
| Child | Female | Skoura | 115.4 | 24.7 |
| Child | Male | Tighfist | 125.1 | 25.7 |
| Child | Female | Tighfist | 121.6 | 26.2 |
Discussion
The first objective of this study was to compare the Skoura Oasis population located in the desert of Morocco to the population in Tighfist of the High Atlas Mountains. We compared BMI and blood pressure between the two rural populations. First, the adults of both populations were compared to one another. In Tighfist in 2009 and 2010, the majority of the individuals that visited the clinics were considered underweight according to international BMI classifications. However, the data collection from 2012 in Skoura classified most individuals as having a normal BMI. Finally, in the data collection from the 2014 Skoura service-learning program, the majority of the males were normal and the majority of females were overweight. These statistics demonstrate a continued need for concentration on malnourishment in places like Tighfist in future service-learning programs. On the other hand, these comparisons show that the Skoura Oasis could benefit from education on exercise, diet, and healthy choices.
The children who were included in the data collection were classified as a certain percentile based on international averages for BMI (Figure 5,6 and 7). When a child is seen at a doctors’ office in the U.S., the physician will use BMI as a way to assess the child’s body composition and health. Physicians categorize children by BMI into the following classifications: underweight (≤ 5th percentile); healthy (5th-85th percentile); overweight (>85th-95th percentile); obese (> 95th percentile). These rankings provide a guide for the doctor to classify children.
In the Tighfist and Skoura Oasis populations, the Tighfist children would be considered healthy because the majority rank within the 25th and 50th percentiles. However, the children in Skoura, especially the males, rank on the lower side of BMI and are considered to be underweight by national standards. These findings are intriguing because most of the adults that we have studied are the opposite based on location (Tighfist adults being underweight and Skoura adults being overweight). These collections show us that aging could affect the development of an individual; therefore, people of all ages in these areas need to be educated on proper diet and exercise. It is possible by speculation that the children in Tighfist are encouraged to eat more than their parents, and may have the potential for being underweight in the future. Therefore, we should educate them on maintaining a healthy weight so they do not deviate from that in the future. On the other hand, it seems as though adults in Skoura are overweight while their children are considered to be mostly underweight. Future programs could educate parents on how to nourish their children, while also trying to improve their own health.
The second objective of this study was to compare height of children and adults from these populations to that of national and international values to evaluate the possibility of malnourishment in these populations. Average heights were generated for each gender in Tighfist and Skoura (Table 3). The average height for adult women in Morocco is 158.5 cm and 172.7 cm for adult males (Female and Male Average Height, 2014). Based on height, both populations are below average when compared to the rest of Morocco. However, Tighfist is significantly lower in height than the national average. Since there is no current information as to why these individuals are so short in stature, we cannot make any conclusions. However, these averages could indicate an increased risk for diseases related to cardiovascular defects or abnormalities (Ha). In future programs, we can record past medical history related to heart disease or abnormalities as an indicator of an association between stature and defects. Short stature could also be due to malnutrition in these areas, specifically Skoura. Because these children may be malnourished, this could increase their risk to be below average height in the future.
This study also aimed to compare the health of Moroccans in the Skoura Oasis to the health of Moroccans in Tighfist. BMI was calculated for all populations (figures 1,2,3). Blood pressure was also compared between Tighfist and Skoura (figure 4a, 4b, table 2).
A condition that has been studied in Morocco is Metabolic Syndrome (MetS). MetS is a cluster of risk factors for diabetes and cardiovascular diseases that include central obesity, hypertension, glucose intolerance, high triglyceride, and low-density lipoprotein cholesterol. This condition is increasing worldwide (Brini et al., 2014). A study conducted on a sample population in Morocco revealed the prevalence of MetS in Moroccan adults. The individuals in the study were classified by age and gender. This investigation found that the prevalence of MetS for males was 18.56% and 40.12% for females. The data showed an increase in Metabolic Syndrome with age. This study found that the average prevalence of MetS (35.73%) was consistent with the U.S. and India, but was much higher than the total South African population. The most prevalent component of MetS in Morocco was abdominal obesity. Although our students in Morocco did not measure abdominal obesity, we can use these standards as a basis of comparison through BMI calculations.
Three risk factors that are evaluated when an individual has the potential for MetS are blood pressure, waist circumference, and blood glucose (Brini et al., 2014). Although blood pressure was the only one of these factors that we evaluated, we can determine the potential for MetS in Tighfist and Skoura based on blood pressure. In the 2009 and 2010 Tighfist data collections, 73.3% of men were hypertensive and 0% of women were hypertensive. This collection included a sample size of 25: 15 males and 10 females. Although this sample size is small, these percentages show that male individuals in Tighfist may be at a higher risk for Metabolic Syndrome because of elevated blood pressure. In future programs, it will be important that the students educate all of the adults, men especially, on the importance of diet and exercise to reduce blood pressure and reduce the risk for MetS. This sample size is based on the people who visited the clinic when Lock Haven was in the area of Tighfist.
In the Skoura data collection from 2012 and 2014, 52.3% of males and 28.5% of females were hypertensive. Therefore, the individuals in this study would be at a higher risk for Metabolic Syndrome and would also need to be educated on a healthy diet and exercise to decrease blood pressure. The sample size for this statistic was 386 individuals: 300 females and 86 males from the 2012 and 2014 service-learning programs.
In future programs, it is important that at least three of the known MetS risk factors be assessed: waist circumference, triglycerides, HDL cholesterol, blood pressure, and glucose. Because it is hard to test triglycerides and cholesterol in a rural primitive clinic, it would be most realistic for future program participants to obtain data on blood pressure, waist circumference, and glucose to determine the prevalence of MetS in the region they are serving. Through this data, many more conclusions can be drawn about the individuals of Morocco. Also, future assessments can strive to be more efficient in recording gender, age, and essential values on all individuals. Based on these collections, we will be able to further study Metabolic Syndrome and other diseases related to overall health in the individuals in Morocco.
The World Health Organization (WHO) has evaluated noncommunicable diseases (NCD) in Morocco. NCD are diseases that are not passed from person to person. They are slowly progressing, long duration diseases that can be the result of high blood pressure and obesity (Noncommunicable diseases, 2014). Elevated blood pressure has been found to be prevalent in 31.2% of males and 33.6% of females that were included in their study and this puts them at a greater risk for chronic diseases (Noncommunicable diseases, 2014). In 2002, the WHO found that chronic diseases accounted for 69% of all deaths and 106,000 people died due to the consequences of chronic disease. The majority of these deaths were due to cardiovascular disease and diabetes. Later, in 2008, the WHO found that there were 209,000 deaths related to NCDs as a result of high blood pressure and obesity. This increase in the number of deaths from 2002 to 2008 is significant. Obesity has also been found to be a risk factor for NCDs in 10.5% of males and 21.9% of females in Morocco in 2008 (Country Profiles, 2014). In 2005, the WHO predicted that 37% of men and 63% of women in Morocco would be overweight. As we approach 2015, this organization predicts that 37% of men and 68% of women in Morocco will be overweight (The impact of chronic disease, 2002).
The WHO has investigated NCDs and found that raised blood pressure and obesity are a precursor to developing a noncommunicable disease (WHO: Noncommunicable diseases, 2014). As described above, hypertension is a main concern for men in Tighfist and for both men and women in Skoura. These factors could put the individuals in our study at a higher risk for developing a noncommunicable disease resulting in a diagnosis of diabetes or cardiovascular disease. In future programs, we can assess noncommunicable diseases and how to prevent them.
When evaluating an individual’s amount of fat, we use Body Mass Index. Although this method does not take into account lean body mass, it is used as a basis for comparison. For the Tighfist 2009 data collection, 75% of males and 93.3% of females were underweight. This demonstrates that these individuals need to be educated on proper nutrition and the essentials to a fat-building diet. In future programs, an assessment of their availability of nutritious foods needs to be accounted for and documented. Once we know what kinds of food they have access to, we can encourage certain amounts of each. The second Tighfist data collection from 2010 also supports the generalization that most of these individuals are underweight because 66.7% of males and 57.1% of females were considered underweight. These individuals would have a lower risk of a noncommunicable disease because they have a lower body weight and most likely a lower waist circumference. This could be due to the fact that there is limited health care being provided to these individuals because they are in such a remote location. Tighfist is located in the High Atlas Mountains of Morocco, as mentioned earlier. These individuals are mostly Berber, an ancient culture of Morocco. They rely heavily on subsistence farming and a central well to obtain food and water. The Berbers of Tighfist refer to the Atlas Mountains as “Mountains of Mountains.” It could be that because of all of the walking and climbing these individuals do, this could be considered their exercise, which is a positive benefit to decreasing noncommunicable diseases.
On the other hand, the individuals that were studied in Skoura in the years 2012 and 2014 would not be at a very high risk for noncommunicable diseases if BMI were the only risk factor. Most of the individuals from this collection were classified as normal based on Body Mass Index. However, there are also a significant amount of individuals, 18.5% of males and 29.2% of females that were overweight from 2012 and 18% of males and 38.2% of females considered overweight in the 2014 collection. These individuals could be at a higher risk for noncommunicable diseases based on their BMI. The Skoura Oasis is located in the deserts of Morocco, very far from any populated city. These individuals rely heavily on subsistence farming and have limited access to clean water unless it is brought in from the city in water bottles. This population is known for consuming large amounts of bread and sugary tea. Because of this, it is important that these individuals receive education on exercise and healthy diet in the future so that the percent of individuals that are overweight does not increase. They should be encouraged to consume the vegetables that they grow from their home, and limit their bread intake in future programs.
Finally, the last objective of this study was to compare the health of the Moroccans in Tighfist and Skoura to the health of Americans based on BMI, blood pressure, weight, and height. In America, 69% of adults over the age of 20 are overweight or obese based on BMI. For children in America ages 6-11, 18% are obese and 18.4% of adolescents are obese (Centers for Disease, 2014). In the data collections from Tighfist, most adults were underweight, and most of the children were considered to be a healthy weight based on BMI. In Skoura, most of the adults were normal or overweight and most of the children were classified as underweight or healthy weight. Therefore, Moroccans in Skoura could be considered more similar to Americans than the individuals in Tighfist based on BMI.
When assessing hypertension in the United States, in 2012, 30.6% of males and 29.3% of females were hypertensive. Our data collection shows that males in Tighfist are significantly above American men at 73.3% hypertensive, and women are below average when compared to American women because 0% were found to be hypertensive. In Skoura, 52.3% of men were hypertensive, which is higher than American men, and 28.5% of women were hypertensive, which is parallel to American women. These studies differ greatly in that American studies are based on a large population of Americans, while the data collections in this study are limited to the small, remote populations.
Next, we were able to compare average weights of American adults to average weights of Moroccan adults from Tighfist and Skoura. The average weight for an American male is 88 kg and 75kg for an adult female. The average weight for a Skoura male is 64 kg, and 60 kg for a female. In Tighfist, the average weight for a male is 39.8 kg and 39.7 kg for an average female (Centers for Disease: body measurements, 2012).
Finally, when comparing average heights of adult Americans to adult Moroccans, we see that Moroccans are shorter in stature. The average height for adult males in America is 176 cm and 162 cm for females. In Tighfist, the average height for adult males is 141 and 139 for adult females. In Skoura, the average height for adult males is 166 cm and 155 cm for females.
All of these differences between Americans and Moroccans can be due to a number of factors. Americans have greater accessibility to potable water, while Moroccans sometimes have to travel to get water from a well or a water bottle that is bought in a store. Americans also have increased access to fatty foods, while Moroccans rely on their own farming and harvesting to sustain their families. Based on this research, we are able to see differences in well-developed countries, such as America, and under-developed countries, such as Morocco.
Conclusion
This study found that the Skoura Oasis and Tighfist are very different populations even though they inhabit the same country. Based on BMI, Tighfist adults were mostly underweight and Skouran adults were mostly normal/overweight. The children of Tighfist were mostly healthy based on BMI and the children of Skoura were mostly underweight/normal. Tighfist and Skouran people have a below average height as compared to the rest of Morocco, and average heights from these populations were below average heights when compared to the American population. Men were more hypertensive in both populations than females, and average blood pressure was lower in Tighfist than in Skoura. Finally, these two populations are both at risk for developing Metabolic Syndrome and noncommunicable diseases. As for Tighfist in the High Atlas Mountains and Skoura Oasis in the Sahara Desert, there is no previous specific research about these rural populations. This study opens doors to further research on these adults and children. In trips following this study, Lock Haven University has the opportunity to begin to identify and reduce the risk for Metabolic Syndrome and noncommunicable diseases by collecting more data on waist circumference, tobacco use, age, blood glucose, past medical history and much more. Through planned education and health care clinics during these trips, we can work to improve the health of the Moroccans in Tighfist and Skoura.
References
Berraho, Mohamed, Youness El Achhab, Abdelilah Benslimane, Karima EL Rhazi, Mohamed Chikri, and Chakib Nejjari. (2013). Hypertension and Type 2 Diabetes: A Cross-sectional Study in Morocco. Retrieved from (http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3343680/)
Brini, Otmane El, Omar Akhouayri, Allal Gamal, Abdelhalem Mesfioui, and Bouchra Benazzouz. (2014, May). Prevalence of Metabolic Syndrome and Its Components Based on a Harmonious Definition among Adults in Morocco. National Institutes of Health. US National Library of Medicine. Retrieved from (http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4124051/).
Centers for Disease Control and Prevention: Body Measurements. (2012, November) Retrieved from (http://www.cdc.gov/nchs/fastats/body-measurements.htm)
Centers for Disease Control and Prevention: Obese and Overweight. (2014, May). Retrieved from (http://www.cdc.gov/nchs/fastats/obesity-overweight.htm)
Female and Male Average Height by Country. (2014). Retrieved from http://www.averageheight.co
The Impact of Chronic Disease in Morocco. (2002). Retrieved from (http://who.int/chp/chronic_disease_report/media/impact/morocco.pdf)
Knoema: Morocco. (2014, May). Retrieved from http://knoema.com/AfDBSED2014Jan/afdb-socio-economic-database-jan-2014?region=1000290-morocco
Noncommunicable Diseases Country Profiles 2014. (2014, July). Retrieved from (http://www.who.int/nmh/publications/ncd-profiles-2014/en/)
WHO: Noncommunicable Diseases Fact Sheet. (2014, March). Retrieved from (http://www.who.int/mediacentre/factsheets/fs355/en/)
World Health Organization: Health System Profile Morocco. (2006). Retrieved from (http://apps.who.int/medicinedocs/documents/s17303e/s17303e.pdf)