DUI Court: A Cross Case Examination of High Risk DUI Offenders
Tyler Reck
Lebanon Valley College
Keywords: DUI, high-risk offenders, typology, CAGE Index, treatment
Abstract
A considerable amount of evidence has been found showing that treatment courts that identify "high risk" and "high need" offenders—those at risk for failure in standard correctional rehabilitation programs (Marlowe, 2012)—are significantly more effective than those who do not. A local DUI Court program had been operating without risk profiling. The purpose of this study was to assist the program in building an easy to implement risk profile assessment strategy using existing measures, including GAGE, mental health status, and stress. Implications for improved targeting of high risk/high need cases are discussed.
Introduction and Literature Review
Driving under the influence (DUI) is a crime that substantially impacts society; according to Mothers Against Drunk Driving (MADD) there were 10,322 fatalities in 2012 (MADD, 2013). A variety of strategies have evolved in order to address this problem, including DUI courts. DUI courts offer an alternative to incarceration, focusing on ending the cycle of continuously being arrested and released due to addictive habits. Following the model of drug courts, DUI courts address underlying alcohol problems of repeat DUI offenders through continuous and frequent judicially supervised treatment, periodic alcohol and drug testing, the use of graduated sanctions, and other appropriate rehabilitative services. A DUI court is composed of a team comprised of a judge, court personnel, probation officials, and treatment providers who meet regularly to assess offender progress (Fell, Tippets, & Langston, 2011). This intensive program helps to break the cycle of addition, lowers DUI recidivism rates, and benefits the community due to specialty court cost effectiveness.
Because not every DUI offender has the same characteristics, it is important for the success of the program that treatment for individuals be tailored to their specific needs. Drug courts that employ risk profiling for offenders are more successful than those that do not employ these profiles (Marlowe & Festinger, 2008). Because drug courts have been in existence much longer than DUI courts, and the profiles of DUI offenders are not nearly as well developed as drug offenders, analyzing the available drug court research is essential to the development of an easily applied high risk DUI profiling model.
DUI Court Research
The research on the effectiveness of DUI courts suggests a range of outcomes. Some studies suggest that these courts are not effective in lowering DUI recidivism. For example, Cavanaugh and Franklin (2012) compared the graduates of a Texas driving while intoxicated (DWI) court to offenders who finished a probation sentence. The two groups were measured at both 6 and 12 month follow-ups; new DWI arrests were analyzed. The results did not produce a favorable view of the specialized court program, as DWI court graduates had higher re-arrest rates after both follow ups, although this difference was not statistically significant. These findings stress the importance of further research on the effectiveness of such programs.
Other findings suggest, however, that DUI court programs experience a significant amount of success. Georgia began its DUI court program by establishing three programs in Chatham, Clarke, and Hall counties in the spring of 2002. As of 2006, 1,053 offenders were admitted to the three DUI courts, and Fell, Tippets, and Langston (2011) found that 301 (29%) had graduated from one of the programs, 532 (51%) were still participating in a program, and 220 (21%) had either not complied with the restrictions or were removed for other reasons. Program graduates also had a 65.1 percent lower recidivism rate than those whose participation was terminated. These data indicate that DUI court does help participants achieve a significant lifestyle change.
What could contribute to more reliable outcomes for DUI courts? In a meta-analysis regarding the cost-effectiveness of drug courts, Bhati, Roman, and Chalfin (2008) determined a 221 percent investment return for every dollar invested. Marlowe (2010) found an even greater percentage when higher-risk offenders were targeted, with a turnaround of 336 percent. Marlowe and Festinger (2012) also found that separating the high risk from low risk offenders can have a significant impact as well. They found that less frequent court appearances for low-risk offenders did not significantly affect graduation or recidivism rates. It was also suggested that an attendance decrease prevented these individuals from becoming susceptible to the negative behaviors and patterns of high-risk offenders.
In order to further define what it means to be a high-risk individual, Marlowe (2012a) distinguished higher prognostic risk and high criminogenic need. He described those with high prognostic risk as those who have a much smaller chance of success in typical rehabilitation programs and criminogenic need as functional impairments that when treated could reduce the prospect of engaging in criminal behavior (Andrews & Bonta, 2010). Following his identification of what a high-risk/high-need offender is, Marlowe (2012b) developed a plan for treating such offenders. He stated that participants in a drug court program should attend court frequently to review progression and consequences, attend substance abuse treatment, be exposed to pro-social and adaptive habilitation, focus consequences on treatment and supervision, and take prescribed medication when needed.
Some research is focused on the characteristic patterns of high-risk offenders. Beck, Ahmed, and Farkas (2012) compared DUI offenders with a low perceived risk of arrest to those with a high perceived risk of arrest. Findings showed that those offenders who believed in a low probability of being taken into custody were more likely to encounter other aggressive drivers, disobey traffic signals, have an acquaintance with a DUI, and have been told they've had too much to drink to drive safely.
Developing profiles for high- and low-risk offenders requires an examination of factors that contribute to such effects. First, the influence of depression was analyzed for its impact among DUI court participants. Thomas, Nochajski, Stasiewicz, and Patterson (2013) studied the role of depression among court-mandated offenders' attitudes. Using a 32-item questionnaire regarding individuals' readiness to change their behavior, individuals with a high level of depression were much more likely to enter a treatment program. Moreover, this may indicate that high-risk offenders show low levels of depression which if placed in a DUI court program could lead to a lack of effort towards a successful graduation.
Furthering the examination of high-risk offenders, Cooper, Russell, Skinner, Frone, and Mudar (1992) analyzed the influence of stress and its moderation of alcohol consumption. By using qualitative interviews to compare this cause and effect relationship, effects directly caused by environmental stressors were found to have a minimal influence. Furthermore, Cleveland and Harris (2010) studied the relationship between negative affect and social experiences and cravings. Findings revealed that day-to-day substance abuse cravings could be accurately predicted by negative triggers.
The characteristics of high risk offenders were further examined though California's 36 drug court programs. Participant characteristics were determined during assessments upon admission into the programs. Results showed that high-risk offenders were significantly more likely to be younger, female, receive mental health treatment, have a higher number of arrests, and a greater number of convictions than low risk offenders (Evans, Huang, & Hser, 2011).
The DUI court program examined for this study currently does not distinguish specialized tracks for high/low risk offenders; consequently it is necessary to identify and develop profiles in order to meet individual needs. Although much research has examined the individual characteristics of high-risk drug offenders, few studies have specifically analyzed those of high-risk DUI offenders. Using the patterns identified for drug offenders, the purpose of this study was to develop an explicit typology of a typical high risk DUI offender. Previous research showed that it is individuals with an addiction, and who either have mental health and/or a high level of stressors, that could be classified as a high-risk individual.
Lebanon County DUI Court
Located in the Commonwealth of Pennsylvania, the Lebanon County DUI Court was introduced in 2008 in part because of the steady increase of DUI offenses from 2003 to 2007. Lebanon was the only county that when compared to other fifth-class counties, did not see a decrease in the number of DUI arrest during this time period. There was a 26 percent increase (397 to 535), for example, in the number of Court Reporting Network (CRN) Evaluations conducted in the county from 2005 to 2007. The 2004 change to the "DUI/Driving after Imbibing" statute may be one explanation for these numbers. The modifications to the statute certainly contributed to the increased jail and prison populations due to the more stringent stance on mandatory incarceration period for second- and third-time offenders. In November 2007, the Lebanon County Correctional Facility (LCCF) had a bed capacity of slightly more than 490 but contained an inmate population of 612.
In addition, second- and third-time DUI offenders in Pennsylvania were to receive prison time even for the lowest allowable BAC of 0.08 percent. The average number of people with one (1) prior DUI violation during the years 2005 to 2007 in Lebanon was 80, while the average number with two (2) prior DUI violations during the same period was 25. From 2002 to 2006, Lebanon experienced 718 alcohol-related crashes—31 led to fatalities.
Lebanon County is a fifth-class county that encompasses a large rural community and contains a city of approximately 24,000 people. The total population is approximately 133,000. The DUI court client population is drawn from all areas of the county. The Lebanon County DUI Court is a post adjudication program that requires offenders to enter a guilty plea to charges and is designed for adult offenders (See Figure 1).
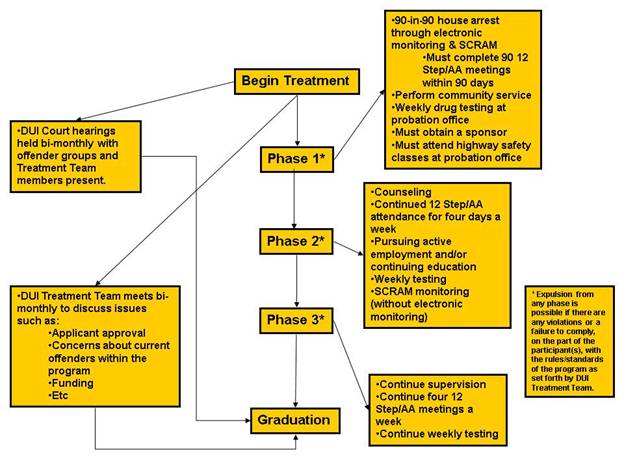
Figure 1. The DUI Court Process From Beginning to End of Treatment
Method
Participants
As of January 2014, 100 male (n = 72) and female (n = 28) DUI offenders were participants within the Lebanon County DUI Court program of Pennsylvania. This program accepts second-time offenders with a blood alcohol content (BAC) equal or greater than .16 percent and third-time offenders with the maximum BAC allowed by law at .08 percent.
Procedure
Three criteria were developed to distinguish high- and low-risk offenders within the program. The CAGE index was employed for creating this profile. Achieving a score of 2 or higher categorized an individual as a high-risk offender. The CAGE index, created by Dr. John Ewing (Ewing, 2008), is a screening tool used to identify problem drinking and is composed of four questions: "Have you felt you should cut down on your drinking?" "Have people annoyed you by criticizing you about your drinking?" "Have you felt guilty about your drinking?" and "Have you had a first drink in the morning to steady your nerves or get rid of a hangover?" Ranging from 0-4, any response of "yes" added a point to one's overall score. Based on these scores, 65 offenders were recognized as high risk.
A mental health index was used consisting of the questions: "Have you ever thought about harming yourself?" "Have you ever thought about harming others?" and "Have you ever attempted suicide?" Scores ranged from 3-6 with an answer of "no" adding 1 point and an answer of "yes" adding 2 points; lower scores indicated mental health issues.
Moreover, a total stress index was also used to compile a sum of the entirety of an individuals' stress. These stressors included: finances, family, friends, general relationships, romantic relationships, work, school, health, crime, alcohol, and drugs. Each type was rated on a 1-5 scale with total scores ranging from 11-55. Finally, several background questions were included such as employment status, age, sex, and prior record.
Data were analyzed using the Statistical Package for the Social Sciences (SPSS). This analysis included descriptive statistics and independent-sample t-tests. The independent sample test was used to compare dependent variables of the high-risk offenders with those of the low risk offenders.
Results
To measure high-risk alcohol abuse and dependence, the CAGE Index was used. Results showed that 65 percent of participants were problem drinkers (n = 65). This suggested that DUI court is targeting DUI offenders facing drinking issues. These high-risk offenders were more likely to be middle aged (M = 38.2, SD = 12) than those in the low-risk group; the difference was significant at the .05 level (See Figure 2). Higher rates of employment were found for individuals classified as low-risk than high-risk; however, it was not significant, p = .051. Similarly, high-risk individuals were more likely to have more prior offenses, although this was also not significant, p = .054.
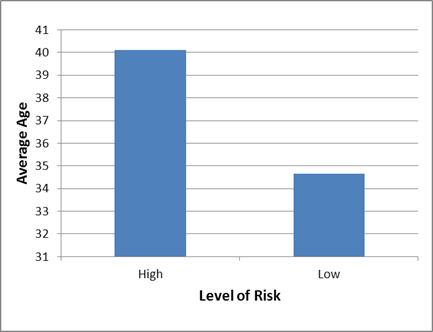
Figure 2. The average age of individuals within the DUI Court program, categorized by level of risk.The next phase of creating the profile was to examine the mental health and stress of this high-risk group. The mental health index was employed to identify the presence of any psychological issues among the high-risk group, and found that 73 percent (n = 73) of the individuals did not display any mental health issues. However, 35 percent (n = 23) of those categorized as high risk, scored a 5 or higher on the index, indicating that more than a third of the participants in question experienced some form of mental health issues. It was also revealed that of those who provided complete responses to the index, 62 percent scored a 2 or higher on the CAGE index.
Participants reported to have experienced some to little stressors on a daily basis (m = 4.1, SD = .59), with lower scores indicating a greater amount of stress. Furthermore, participants categorized as high risk reported experiencing slightly more stressors than those with a lesser classified risk (See Figure 3). This difference was significant (p < .000). This was evident as 38.5 percent (n = 22) who completed the stress index were labeled as high risk and reported feeling stress at least some of the time (≤38).
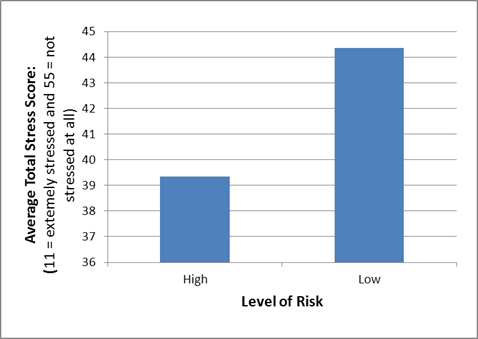
Figure 3. Self-reported stress scores categorized by level of risk.The next step was to examine how effectively the risk-profile predicted recidivism. Among the current group of 100 offenders, 17 (13%) received another charge; this resulted in their removal from the program or it occurred after program graduation. Of these, 7 were identified as high risk. New DUI offenses were only received by 3 individuals; 2 after graduation (high risk), and 1 (low risk) following his/her removal (See Table 1). Furthermore, 1 individual (high risk) was removed due to a new substance use charge and another (low risk) received a similar charge upon completion. One individual labeled as low risk was also charged with public drunkenness after graduating (See Table 2).
Table 1. High-risk offender re-offenses after acceptance into DUI Court
Notes.1 Only one was received following DUI Court graduation and was only charge received after completion.
___________________________________________________ Charges Number of Occurrences ______ ____________________ Driving Under Suspended License 3 Drug Possession 1 New DUI 21 Simple Assault 1 ___________________________________________________ Table 2. Low-risk offender re-offenses after acceptance into DUI Court
___________________________________________________ Charges Number of Occurrences ______ ____________________ Drug Possession 1 New DUI 1 Simple Assault 4 Public Drunkenness 1 Resisting Arrest 1 ___________________________________________________ Discussion
Preliminary results show that the CAGE, Mental Health, and Stress indexes can be valuable screening tools to create profiles of DUI offenders. The CAGE index proved to be the most valuable as it identified individuals who were problem drinkers. A mental health and stress screening assessment has additional potential in creating risk profiles.
Despite the success of these indices, some findings were inconsistent with previous literature. Cooper, Russell, Skinner, Frone, and Mudar (1992) found that stressors causing increased alcohol consumption cannot be generalized to everyone but are specific to the individual. The findings from this study, however, determined multiple stressors that may be influential. Evans, Huang, and Hser (2011) also found that problem drinkers tended to be younger individuals, but high-risk individuals in this study tended to be middle aged. Although there were inconsistencies, many findings were consistent with previous literature. For example, that problem drinkers within the program were found to have more frequent mental health issues is consistent with Nochajski, Stasiewicz, and Patterson (2013). Additionally, successful graduates had a lower recidivism rate, supporting the findings of Fell, Tippets, and Langston (2011).
This study had several limitations. First, the sample size was problematic. Since its implementation, only 100 participants have been admitted to the program and 80 had graduated by January of 2014. Second, the composite index scores must address the problem of missing data. The approach taken for this study was to exclude all cases with missing data. Only 36 offenders provided complete replies to individual items forming the mental health index, and only 57 gave full answers for the stress index. Although useful, future research must consider alternate methods of index construction. This will increase the strength of these indices (Babbie, 2014). Finally, the risk profiles were not employed during offender participation in the court. The profiles should be employed immediately upon program entry so that needs of problem drinkers and those with high stress and mental health problems are appropriately identified.
References
Andrews, D. A., & Bonta, J. (2010). The psychology of criminal conduct (5th ed.). New Providence,NJ: LexisNexis.
Beck, H., Ahmed, A., & Farkas Z. (2012). Characteristics of dui offenders with a high versus low perceived risk of arrest, Traffic Injury Prevention, 14(1), 1-6, 10.1080/15389588.2012.683119
Bhati, A. S., Roman, J. K., & Chalfin, A. (2008). To treat or not to treat: Evidence on the prospects of expanding treatment to drug-involved offenders. Washington, DC: The Urban Institute.
Cavanaugh, M., & Franklin, T. (2012). Do DWI courts work? An empirical evaluation of a Texas DWI court, Journal of Offender Rehabilitation, 51, 257-274, doi: 10.1080/10509674.2011.641074
Cleveland, H., & Harris K. (2010). The role of coping in moderating within-day associations between negative triggers and substance use cravings: A daily diary investigation, Addictive Behaviors, 35 (2010), 60-63.
Cooper, M., Russell, M., Skinner, J., Frone, M., & Mudar, P. (1992). Stress and alcohol use: Moderating effects of gender, coping, and alcohol expectancies, Journal of Abnormal Psychology, 101(1), 139-152.
Evans, E., Huang, D., & Hser, Y. (2011). High-risk offenders participating in court-supervised substance abuse treatment: Characteristics, treatment received, and factors associated with recidivism, Journal of Behavioral Health Services Research, 38(4), 510-525, doi:10.1007/s11414-011-9241-3.
Ewing, J. (2008). The CAGE questionnaire for detection of alcoholism, The Journal of the American Medical Association, 300(17), 1-4.
Fell, J., Tippets, A., & Langston, E. (2011). An evaluation of the three Georgia dui courts, National Highway Traffic Safety Administration, March 2011, 1-63.
MADD (2013). Goals and Strategies. Retrieved from http://www.madd.org/about-us/madd-goals.html
Marlowe, D. (2010). Research update on adult drug courts, National Association of Drug Court Professionals, December 2010.
Marlowe, D. (2012a). Alternative tracks in adult drug courts: Targeting the right participants for adult drug courts (part one of a two part series), National Drug Court Institute, 7(1), 1-12.
Marlowe, D. (2012b). Alternative tracks in adult drug courts: Matching your program to the needs of your clients (part two of a two part series), National Drug Court Institute, 7(2), 1-12.
Marlowe, D., & Festinger, D. (2008). Low-risk offenders do equally well with and without regularly scheduled court appearances, National Institute of Drug Abuse, Retrieved from http://www.drugabuse.gov/news-events/nida-notes/2008/12/high-risk-drug-offenders-do-better-close-judicial-supervision
Thomas, H., Nochajski, Stasiewicz, P., & Patterson, D. (2013) Depression, readiness for change, and treatment among court-mandated dui offenders, Journal of Dual Diagnosis, 9(2), 139-148, doi:10.1080/15504263.2013.779092
Acknowledgements
I would like to thank the Lebanon County DUI Court and District Attorney's Office for the collaboration allowed with Lebanon Valley College. I would also like to thank Destiny Myers for her mentorship and assistance with data collection. Additional thanks to Dr. Marianne Goodfellow for her supervision of this project, as well as to Donna Miller, LVC, Librarian for assistance with references.
|